


Related Flashcards
Related Topics

Cards In This Set
| Front | Back |
|
Cause-and-effect or fishbone diagram
|
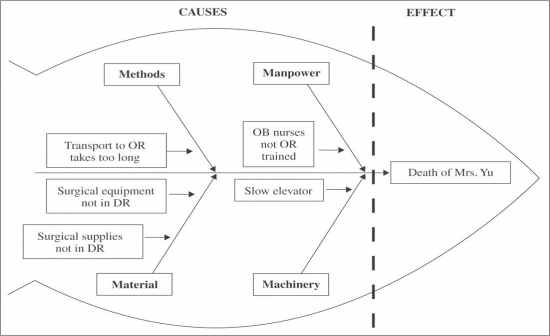 1.Cause-and-effect or fishbone diagram: QI Toolbox Technique used most often in root cause analysis is "Cause-and-Effect" or "Fishbone Diagram" ... This technique structures the root cause inquity and helps the investigators to be sure that they have examined the situation from all perspectives ... An investigational technique that facilitates the identification of the various factors (i.e., Manpower, Material, Methods, and Machinery) that contribute to a problem; also called a fishbone diagram. |
|
(FMEA)
|
2.) Failure mode and effects analysis (FMEA) - A technique that promotes systems thinking, FMEA includes defining high-risk processes using flowcharts; identifying potential failure points in current processes; and scoring each potential failure by considering factors such as the frequency of failure, potential harm, and the likelihood that the failure will be detected before it reaches the patient. Potential failures with the highest criticality score become the focus of process redesign (Joint Commission 2008b)
|
|
Incident Report or Occurence Report
|
3.)Incident Report or Occurence Report: A structured data collection tool that risk managers use to gather information about potentially compensable events; also called an incident report.
|
|
Medication error
|
4.)Medication error: A mistake that involves an accidental drug overdose, an administration of an incorrect substance, an accidental consumption of a drug, or a misuse of a drug or biological during a medical or surgical procedure.
|
|
Incident Report or Occurence Report
|
5.) Incident Report or Occurence Report: A structured data collection tool that risk managers use to gather information about potentially compensable events; also called an incident report.
|
|
(PCEs)
|
6.) Potentially compensable events (PCEs): An occurrence that results in injury to persons in the healthcare organization or to property loss.
|
|
Risk
|
7.) Risk: A formal insurance term denoting liability to compensate individuals for injuries sustained in a healthcare facility.
|
|
Root-cause analysis
|
8.) Root-cause analysis: Analysis of a sentinel event from all aspects (human, procedural, machinery, material) to identify how each contributed to the occurrence of the event and to develop new systems that will prevent recurrence.
|
|
Bloodborne pathogen
|
9.) Bloodborne pathogen: Infectious diseases such as HIV and hepatitis B and C that are transported through contact with infected body fluids such as blood, semen, and vomitus.
|
|
Community-acquired infection
|
10.) Community-Acquired Infection: An infection that was present in a patient before he or she was admitted to a healthcare facility.
|
|
Flowcharts
|
11.) Flowcharts: An analytical tool used to illustrate the sequence of activities in a complex process.
|
|
(HAI)
|
12.) Healthcare-associated infection (HAI): An infection occurring in a patient in a hospital or healthcare setting in whom the infection was not present or incubating at the time of admission, or the remainder of an infection acquired during a previous admission.
|
|
Icons
|
13.) Icons: A graphic symbol used to represent a critical event in a process flowchart... Some Examples: Process Icons, Decision Icons, Predefined Process Icons, Connector Icons, Terminator Icons, Manual Input Icons, or Line Connector Icons.
|
|
(MDROs)
|
14.) Multiple drug-resistant organisms (MDROs): A bacteria of any kind that has become resistant to many different antibiotics.
|
|
Standard precautions
|
15.) Standard precautions: The application of a set of procedures specifically designed to minimize or eliminate the passage of infectious disease agents from one individual to another during the provision of healthcare services.
|
